
Our Model
How Adira worked, and why it was different from typical foundation grantmaking.
Adira's Big Idea
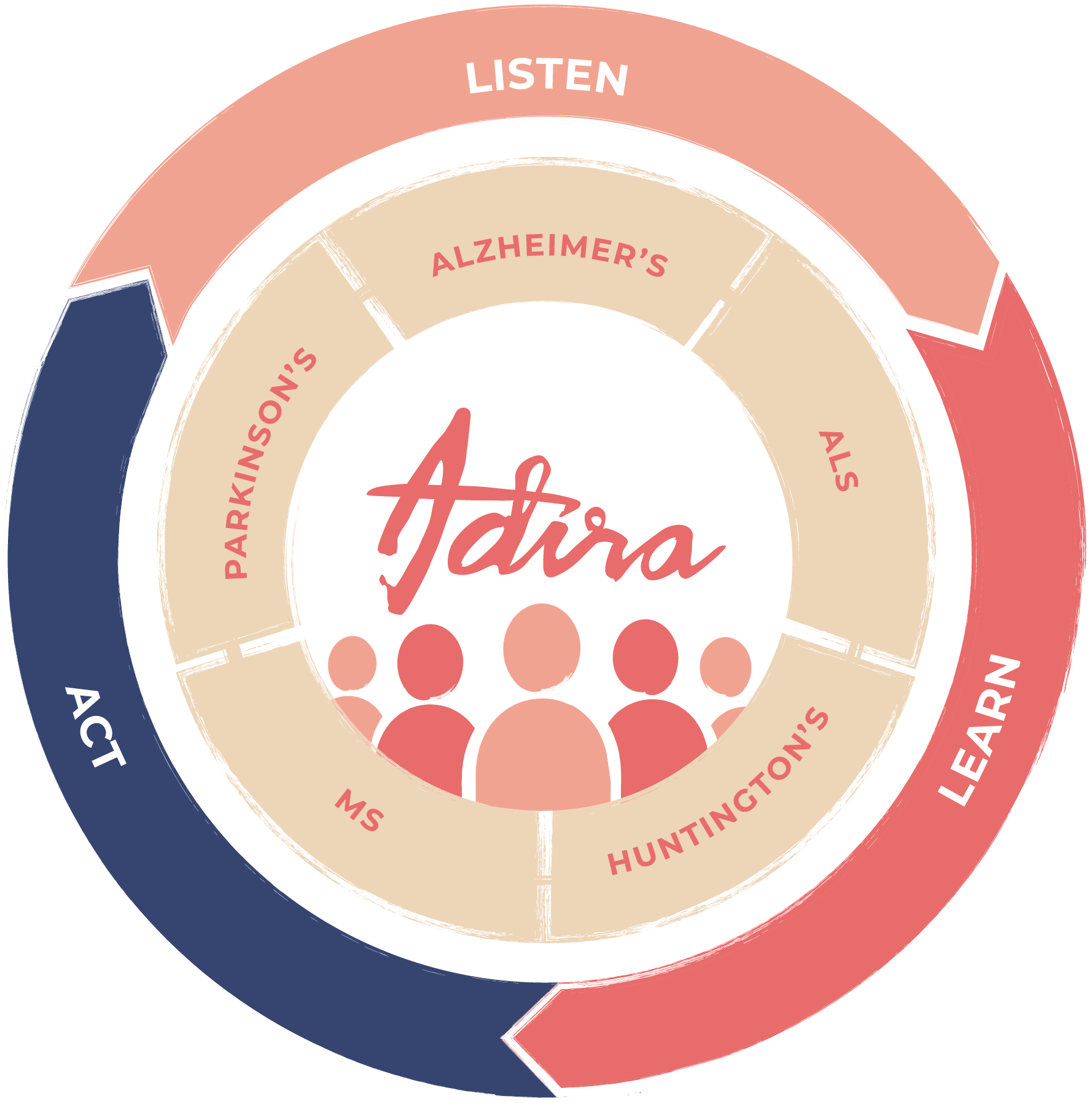
Adira focused on five neurodegenerative diseases as one community: Alzheimer's disease and related dementias, ALS, Huntington's disease, multiple sclerosis, and Parkinson's disease. In the U.S., that was 8 million people in 2020, expected to grow to 11 million by 2030, a 38 percent increase.
Adira's focus was principally, though not exclusively, on these five. Each disease has unique needs. But seen from a bird's-eye view, they share far more in common than not. Mobility. Caregiving. Cognition. Grief. Financial security. Stigma. Mental health. Isolation. The problems that get funded least, if at all, are usually the ones people share across diagnoses.
Adira took this big bite so it could accelerate new ways of collaborative thinking, financing, and community building. "Adira" is an ancient name meaning brave. The work required it.
The Problem We Were SolvingLife had grown isolating for everyone. People who were ill felt it most.
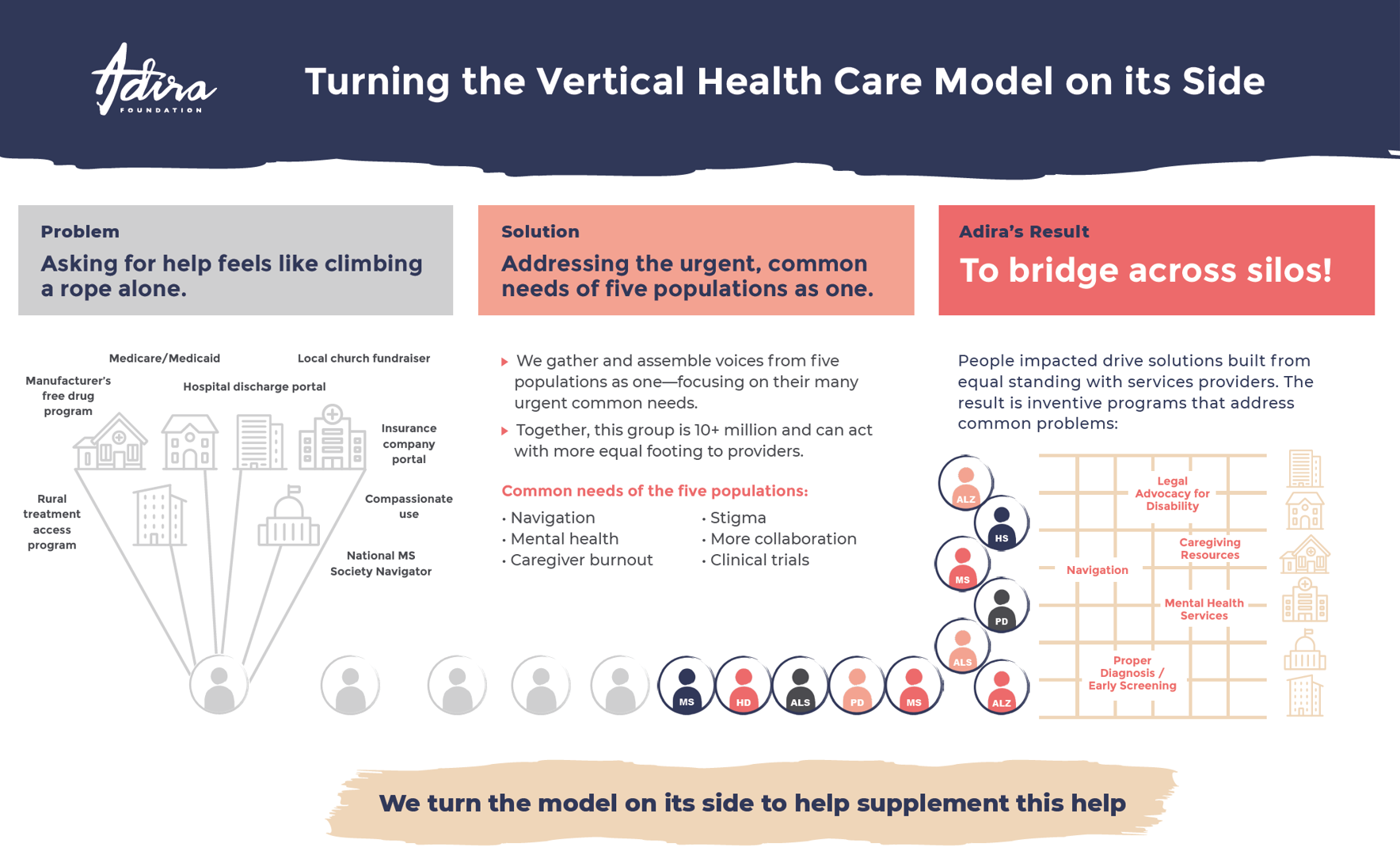
Service providers could not solve everything at once. Many took on one population, one point of view, or one service at a time. Each program was designed in good faith. But every additional program could compound the burden on a person. Finding 17 paths for 17 problems would shut anyone down.
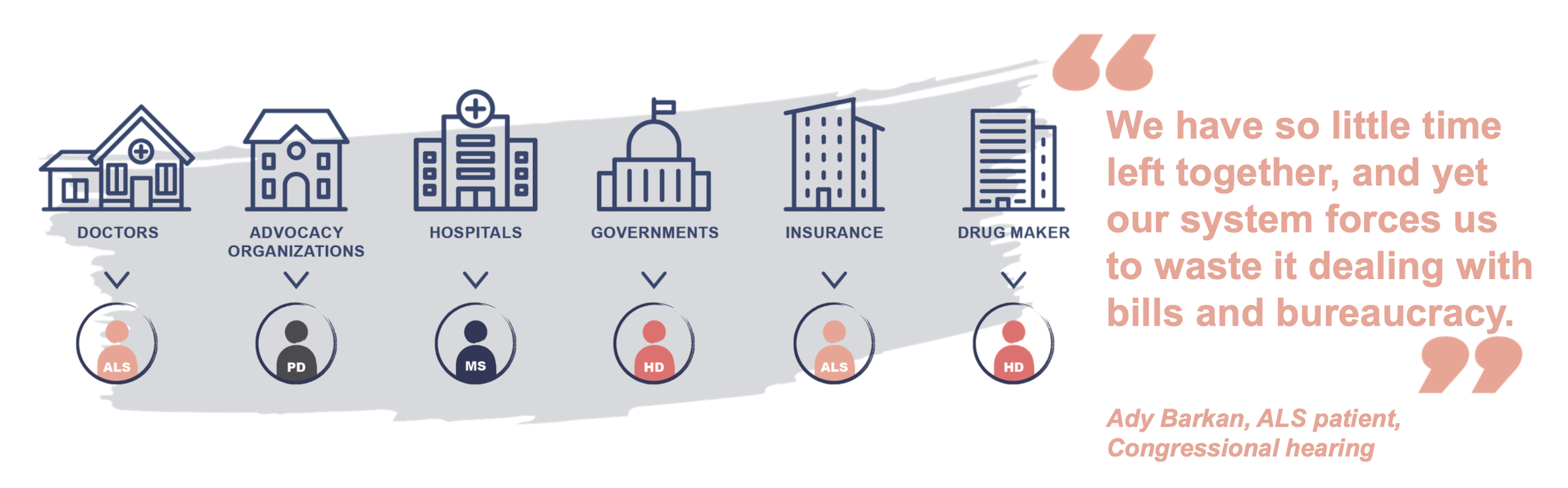
Silos Isolate and Crush Us
"We have so little time left together, and yet our system forces us to waste it dealing with bills and bureaucracy."
— Ady Barkan, ALS patient, Congressional hearingOUR SOLUTIONAdira asked people two questions. What do you still urgently need? And what would good help look like?
Then Adira leveraged funding for nonprofit grants designed for a common, integrated response. Solutions were built from equal standing between the people getting help and the people giving it. The result was inventive programs that addressed common problems across all five disease communities: legal advocacy for disability, caregiving resources, mental health services, proper diagnosis, navigation.
Adira turned the vertical health care model on its side. Instead of one service for one population, the goal was wide, system-level work that addressed the cross-cutting needs typically left behind.
Bridges Across Silos
BEYOND THE BULLSEYEAdira's work rested on three program pillars. Each one fed the others. Together they were how Adira listened, learned, and acted.

Three Pillars of Adira's Work
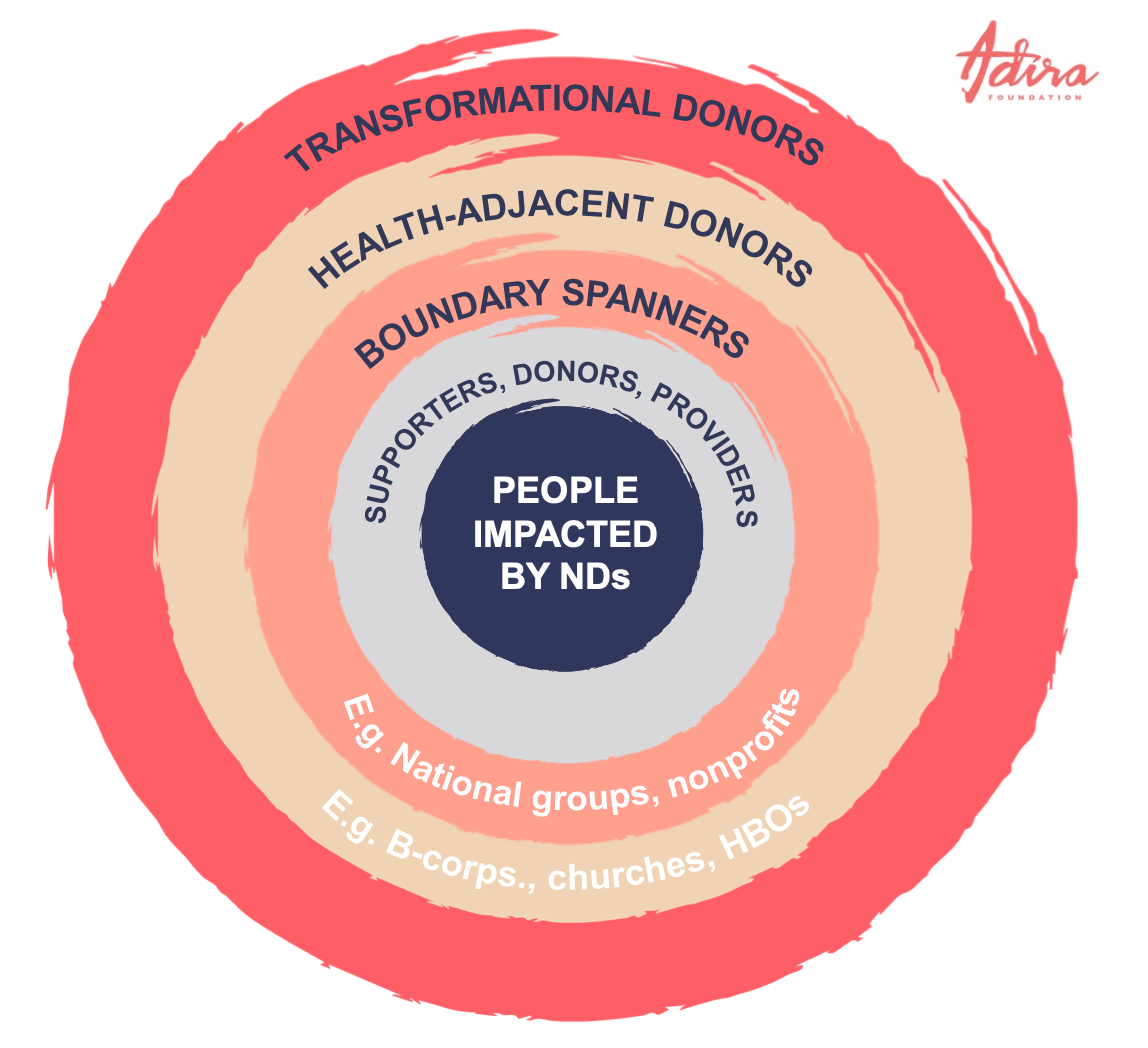
BEYOND THE BULLSEYESingular disease efforts tended to circle in the inner layers of the bullseye: people impacted, their direct supporters, providers, and traditional donors. Adira focused on reaching the outer layers to supplement the inner layers.
That meant boundary spanners, health-adjacent donors, and transformational donors. Sports, entertainment, faith-based organizations, B-corps, venture philanthropists. Adira aimed to reach potential influencers who were unlikely to stand with one singular disease, but who might stand with 8 million people across five diseases for a larger purpose of collaborative reform.
Adira convened these groups on neutral platforms. The aim was community-driven priority setting, movement building, and larger financing mechanisms that brought results-based financing, accountability, oversight, leverage from other sectors, and economies of scale.
Beyond the Bullseye
OUR NORTH STARAdira was inspired by the ambition, scale, and scope of successful integrated responses to other health challenges:
The Ryan White Program
The U.S. President's Emergency Plan for AIDS Relief (PEPFAR)
The Global Fund to Fight AIDS, Tuberculosis, and Malaria
Adira applied their best practices. Funded by many. Steered by results. Complementary to other good programs. Informed by what people said they needed.
Five elements shaped how Adira worked: collaborative and additive, objective, community-driven, instructive, and transparent and accountable.
Inspired by Proven Models
COMPARISONAdira's approach was a deliberate departure from how most disease-specific philanthropy operated. Here is what that looked like in practice.
Typical Response
Looked at what made people unique
Person affected as end user
Small but mighty communities swimming upstream
Designed from the point of view of donor or provider
Helpful but limited
Ground level: what was easier to count and fund
Either designed for the individual or for the system
More pressure on any one donor
Targeted to the needs of the few
Person as their sick self
Costly Categorical identity
Traditional donors
Adira's Response
Looked at what made people typical
Person affected as co-collaborator
Larger community turning the tide
Led by the point of view of the person impacted first, then with the donor
Supplementing what already worked
Bird's-eye view for more perspective and impact
Straddling both, the diagonal approach
Diffusion of donor influence and pressure
Targeted to the needs of the many
Person as their best self
Economies of scale
Shared identity
Transformational donors plus traditional donors
How Adira Worked Differently


