
Background Research
Adira's work was grounded in two kinds of research:
what was already known about neurodegenerative diseases, and what Adira commissioned to learn more.
Part One: Why Neurodegenerative Diseases
Five Diseases, One Community
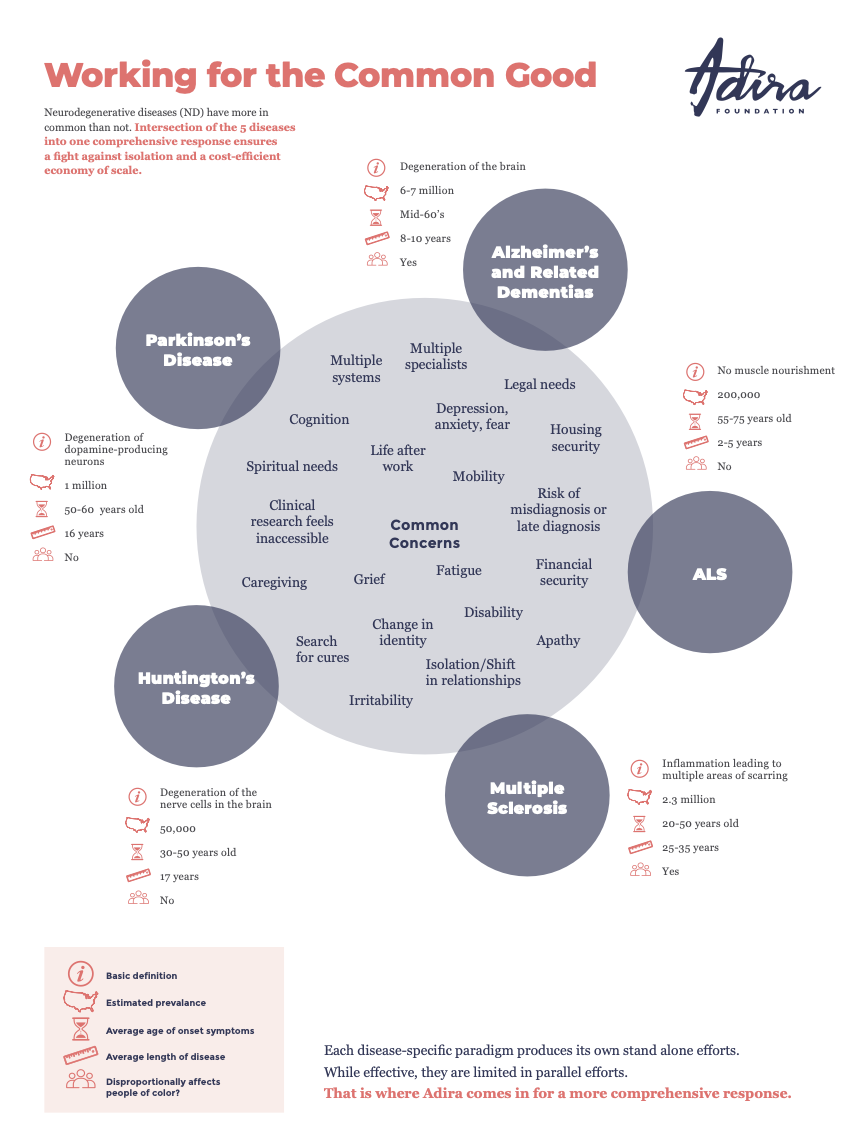
Adira focused on five neurodegenerative diseases that are highly complex and share more in common than not:
Alzheimer's disease and related dementias — degeneration of the brain, 6 to 7 million people in the U.S., average onset mid-60s, disease length 8 to 10 years
ALS (amyotrophic lateral sclerosis) — no muscle nourishment, 200,000 people in the U.S., average onset 55 to 75 years old, disease length 2 to 5 years
Huntington's disease — degeneration of the nerve cells in the brain, 50,000 people in the U.S., average onset 30 to 50 years old, disease length 17 years
Multiple sclerosis (MS) — inflammation leading to multiple areas of scarring, 2.3 million people in the U.S., average onset 20 to 50 years old, disease length 25 to 35 years
Parkinson's disease — degeneration of dopamine-producing neurons, 1 million people in the U.S., average onset 50 to 60 years old, disease length 16 years
Each disease has unique features. But seen together, they share common concerns: caregiving, financial security, housing security, mobility, depression, isolation, grief, legal needs, multiple specialists, search for cures, life after work, change in identity, fatigue, and the risk of misdiagnosis or late diagnosis.
A Rapidly Growing Need
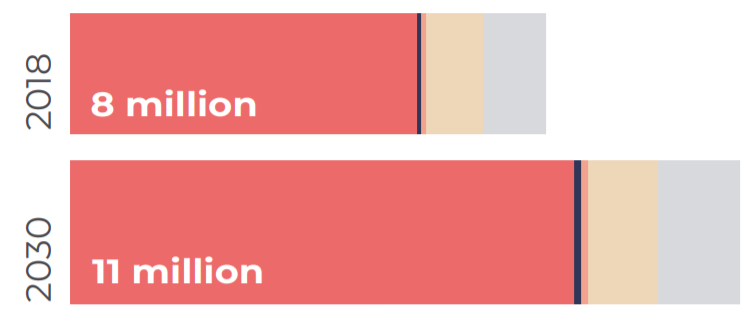
The incidence, prevalence, costs, and burden of neurodegenerative diseases were all growing at an alarming rate. The total number of people living with these five diseases in the U.S. was projected to grow from 8 million in 2020 to 11 million by 2030, a 38 percent increase.
These diseases disproportionately impact the oldest demographic, a population expected to grow to 19 million by 2050. The annual cost to the U.S. health system to treat people living with neurodegenerative diseases was $43.6 billion as of 2017.
What's worse, those dealing with these scary, isolating, complex diagnoses were often those least equipped to handle them.
Programs Designed Without the Patient in Mind
Most programs serving neurodegenerative disease communities were narrowly focused on a discrete issue and designed from the perspective of the provider or programmer, not the patient point of view. When you needed a single service, one well-designed program could be a lifesaver. But when you had a neurodegenerative disease and needed a wide variety of services, navigating the current health care system was paralyzing.
Research showed that family members serving as caregivers were also at risk of significant emotional, mental, and physical health problems. Most caregivers were not fully prepared for the role and received little or no support, resulting in a diminished quality of life for both the caregiver and the patient.
The need for comprehensive and coordinated solutions across sectors and among multiple players was clear. That need is what brought Adira into existence.
Multilateral Funding to Transform Care in Neurodegenerative Disease
In 2020, Adira commissioned faculty at George Washington University's Milken Institute of Public Health to study three successful multilateral health programs: the Ryan White HIV/AIDS Program, the U.S. President's Emergency Plan for AIDS Relief (PEPFAR), and the Global Fund to Fight AIDS, Tuberculosis, and Malaria.
The researchers conducted literature reviews, interviewed experts on those programs, and spoke with professional stakeholders in the neurodegenerative disease community. They identified the best practices that made these programs work and considered how they could apply to a similar model for neurodegenerative diseases.
The resulting white paper, Multilateral Funding to Transform Care in Neurodegenerative Disease, outlined 16 recommendations across two categories: identifying and addressing unmet needs, and engaging other funders.
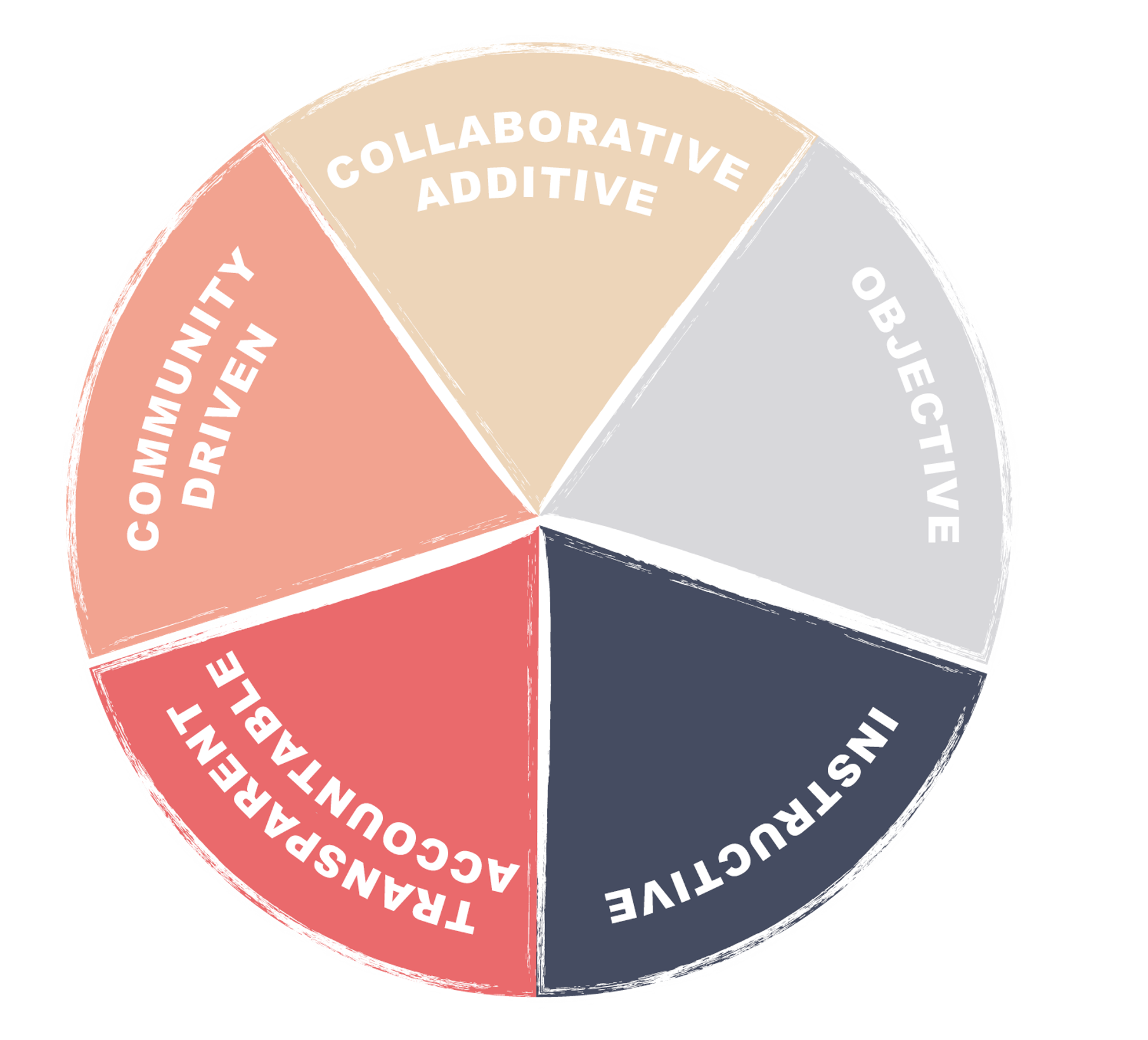
Five key principles emerged from the GWU research as the foundation of successful multilateral approaches:
Community-driven — prioritizes the perspective of the people impacted
Additive, not divisive — makes care more navigable, more communal
Objective and independent — diffuses influence through pooling money and convening
Instructive — improves systems through proven new best practices
Transparent and accountable — brings daylight and uniformity to oversight
Adira built its model on these five principles.
Community Engagement and Outreach for People of Color
Adira recognized early on that amplifying the voices of historically marginalized groups within the ND community was essential. In 2020, Adira engaged GOODSTOCK Consulting to develop a community engagement strategy specifically targeting people of color.
GOODSTOCK conducted focus groups with people of color living with neurodegenerative diseases and their caregivers, and interviewed healthcare providers of color. They produced 15 recommendations for Adira to implement an effective community engagement strategy.
The recommendations were organized into four categories:
Prioritize network mapping and network building
Develop a targeted partnership strategy
Develop and implement engagement opportunities
Deploy targeted communication efforts
These recommendations shaped how Adira approached every subsequent listening session, grant round, and Flagship Project.

Measuring What Matters to People with Neurodegenerative Diseases
In 2021, Adira studied more than 50 existing tools for measuring quality of life. The goal was to understand how the field already measured the things that matter most to people living with ND, and to identify gaps and opportunities for a common standard.
Adira presented the findings at a July 2021 convening attended by professionals from more than 30 organizations.

Mapping the Field
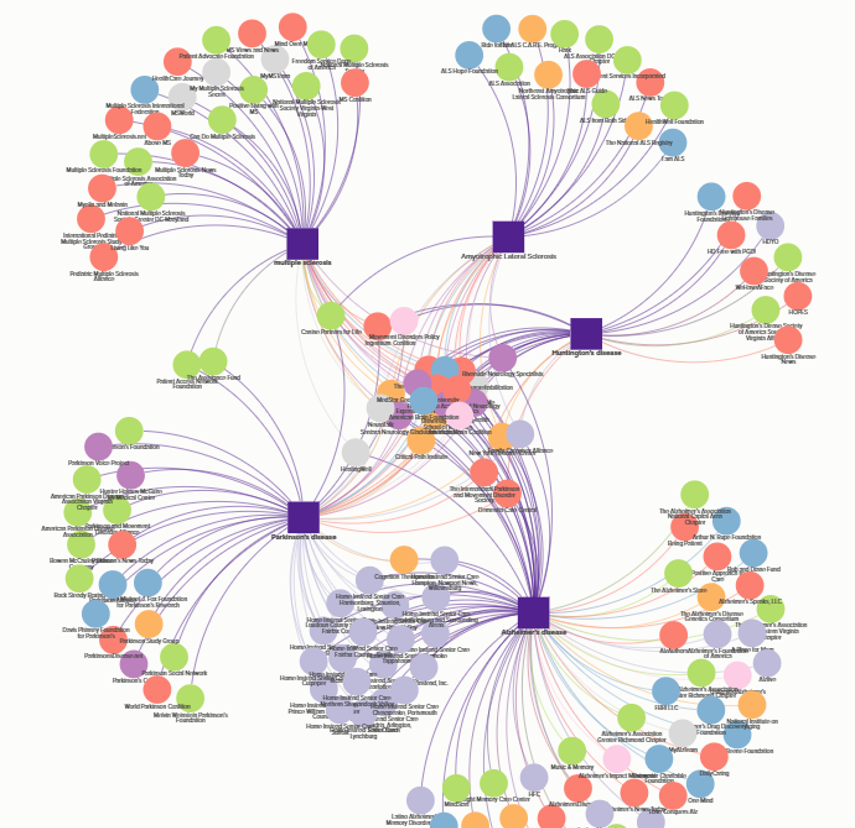
Adira mapped the U.S. organizations serving one or more of the five disease communities. The resulting network map plotted organizations into an interactive, searchable web-based data visualization, used to identify underfunded communities, underserved geographic areas, programming gaps, networking gaps, and collaboration opportunities.
The map made one finding starkly visible: very few organizations worked across all five disease communities. The white space between disease silos was exactly where Adira focused.
What People Said They Needed
Beyond commissioned research, Adira treated listening itself as a research method. Across 2019 to 2022, Adira conducted convenings, focus groups, story collections, and one-on-one conversations with people living with neurodegenerative diseases and their caregivers.
Stat callouts:
40,000+ people reached through Adira's listening and grantmaking
2,000+ people living with ND and caregivers heard from directly
350 people weighed in on Round 2 grant design through convenings, needs assessments, and focus groups
34 Round 2 applications received, 5 funded, 29 non-funded organizations called individually to share feedback
That listening shaped every grant round, every Flagship Project, and the design of the Neurodegenerative Disease Congress.
